How To Take Accurate Blood Pressure Measurements (and what to do with the readings once obtained)
I have been a practicing physician in Washington now for over 40 years. A lot has changed over that time frame. The advances in most fields of medicine have truly been astounding. Back in medical school, we learned just how important blood pressure measurements were in determining risks for cardiovascular disease. To measure blood pressure back then, we used mercury sphygmomanometers (blood pressure cuffs) and for portable use, we used aneroid blood pressure cuffs. That was the state-of-the-art back then. Yes, we had heart catheterizations and bypass surgery, but we did not have stress echocardiograms, high resolution echocardiograms, virtual angiograms, nuclear stress tests, heart scans, PET scans or MRIs to assess cardiovascular health. These technologies along with advances in medications and procedures have allowed us to substantially reduce morbidity and mortality from cardiovascular disease. However, even with all these high-tech changes, it turns out that the accurate measurement of blood pressure is still one of the very most important measurements we take in the assessment of cardiovascular risk. Treatment of high blood pressure (hypertension) substantially reduces the risk of cardiovascular disease. However, we cannot treat hypertension if we do not accurately measure blood pressure, so we really must be doing this correctly.
Like many millions of Americans, I personally have hypertension. Despite living a very healthy lifestyle with a good diet, low salt intake, daily exercise and minimal alcohol consumption, I have to take blood pressure medication. Over the past 20 years, I have gone for all the standard testing including: 3 heart scans, 2 echocardiograms, 1 stress echocardiogram and a carotid Doppler study to assess my level of cardiovascular risk. I have gone for annual physical exams, have had numerous measurements of my cholesterol and other markers of cardiac risk, and have consulted a cardiologist on several occasions. There is only one thing I have not had on any of these visits to the healthcare system – and that is an accurate measurement of my blood pressure!! How can that be???
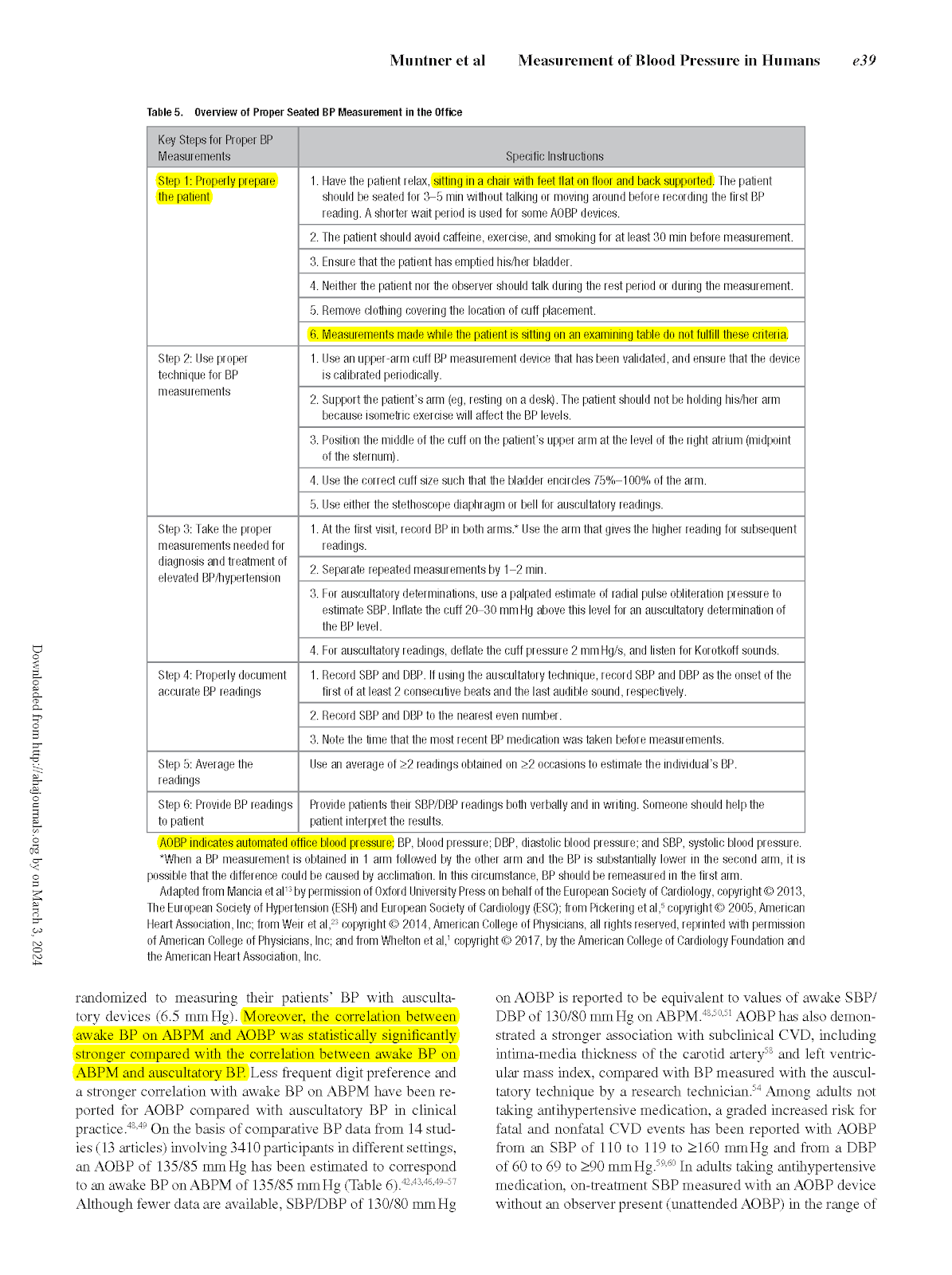
Although we have advanced in the technology of measuring and treating high blood pressure over the past 40 years, it seems as though most physicians are still back in the 1980s as far as their understanding of what constitutes adequate technique for measuring blood pressure. There are well established guidelines about how to accurately measure blood pressure (see Appendix 1). Unfortunately, most physicians either do not know them or they know them and do not implement them. Accurate measurement of blood pressure is done with the patient sitting in a chair, feet flat on the floor and back supported. They are not supposed to be done while you are seated on an exam table, with your feet dangling either dressed or undressed. Automated blood pressure instruments that take multiple readings over several minutes are considered the most accurate way to determine your blood pressure. Let’s face it, measuring and treating blood pressure is all about getting and evaluating good blood pressure data, and eliminating extraneous variables gives us the most valuable information.

If you ask most doctors how they determine if your blood pressure is controlled or not and the goals of blood pressure treatment, they refer to the SPRINT trial (Systolic Blood Pressure Intervention Trial). This trial, published in 2015 fundamentally changed the modern approach to blood pressure evaluation and treatment, indicating that more aggressive treatment of blood pressure, achieving a goal blood pressure of 120/80, substantially reduces the risks of cardiovascular disease, heart attack, heart failure and stroke. This was a major milestone and advance in our understanding and treatment of hypertension.
In the SPRINT trial, decisions about the treatment of high blood pressure were made based on very specific guidelines. The treatment algorithm was based upon accurate measurements of blood pressure done with the guidelines listed in Appendix 1. Patients were seen at regular intervals with blood pressures measured with patients seated in chairs, using automatic blood pressure monitors that recorded 3 readings over 5 minutes, and averaging those readings at every visit (Automated Office Blood Pressure – AOBP). All treatment was based on these blood pressure determinations, and the findings were clear, bringing blood pressure down to 120/80, versus leaving it at 140/90, reduced cardiovascular complications by 25%. The study was so singularly impressive, that most physicians have adopted the new goal for blood pressure treatment in people with hypertension as to target blood pressure readings of 120/80. However, if one is not taking accurate measurements, it is not possible to achieve the benefits clearly outlined in this landmark trial.
When I read the SPRINT trial, I immediately ordered the automated blood pressure monitors that were used in the trial. Since that time, over the past decade, in our medical office at DC Internists, we follow the SPRINT guidelines in measuring blood pressure, and treating to the target ranges as outlined in the trial (Getting all the way down to 120/80 may be hard to achieve in some patients and so we customize the approach based on individual patient characteristics). These monitors are not very expensive, easy to use, and should be implemented in all medical practices that deal with hypertension and its complications. Yet, despite this overwhelmingly popular and scientifically valid landmark study, virtually no clinical medical settings I have visited have adopted this approach. I just cannot understand why.
The Sprint study is not perfect, and there are other ways of obtaining good blood pressure data. We also advocate that our patients do home blood pressure readings on their own. We recommend highly rated home blood pressure monitors such as the Omron series 10 units. These monitors can be easily set up to do readings in the same manner as done in the SPRINT study i.e. 3 readings over several minutes. In addition, when there is doubt about the accuracy of blood pressure readings in certain individuals, we perform home 24-hour blood pressure monitoring. These are more sophisticated portable blood pressure monitors that record your blood pressure every 20 minutes during the day, once an hour at night, and gives us 24-hour trending of an individual’s blood pressure. It turns out that home ambulatory blood pressure monitoring (ABPM) correlates better than virtually any other parameter in assessing outcomes from uncontrolled high blood pressure. These 24 hour monitors are somewhat inconvenient, and we reserve using these for more difficult or complicated cases. We have our own unit and will perform this test on our patients when appropriate.
Obtaining accurate office blood pressure readings with automated office blood pressure monitoring (AOBP) as was done in the SPRINT study, combined with regular home monitoring, is usually adequate information to determine accurate blood pressure readings and helps us determine the best treatment approach for all of our patients. We pride ourselves at DC Internists on being one of the few offices that take the approach to high blood pressure seriously and follow the current guidelines in measuring and treating hypertension. If you have further questions about this, any of our doctors would be happy to discuss this with you.
Mitchell B. Dunn, MD